WCAG Heading
by Philip Jett
It was 1918 and there was a killer on the loose. Worse than any serial predator in modern history, its deadly grasp was swift, its hold resolute, and its thirst for killing unquenchable. No one was safe. It tracked down its victims in their homes and businesses, on city streets and farms. It cared nothing of royalty, wealth, age, race, gender, or national origin. The industrial revolution only encouraged it and modern advances in medicine could do little to slow it. The invisible monster’s name was the Spanish influenza.
With the spring of 1918 came hope. The war in Europe seemed to be nearing an end and that meant an end to the horrible killing. But just as hope came, so did something else. Soldiers on the front lines and back home in military camps began getting sick. Word came from Spain of a flu epidemic within its borders that had even stricken its king. People called the new malady the Spanish influenza, though it likely originated elsewhere.
The Spanish influenza’s first wave spread swiftly during the spring and summer of 1918, but it was a mild strain, killing no more than during a typical flu season. Boards of health reported that the virus affected “most severely elderly persons and others whose powers of resistance are weakened by illness, work, or worry, especially those who are ‘run-down’ or ‘not feeling up to the mark.’”
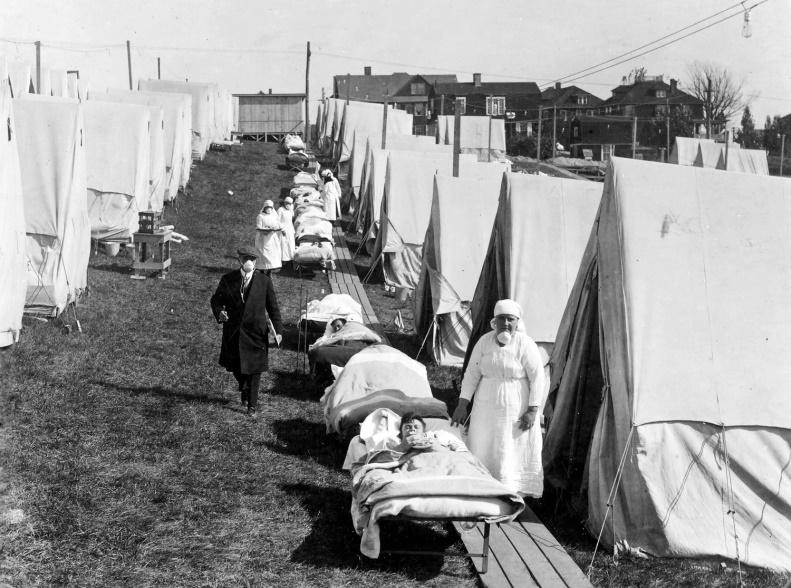
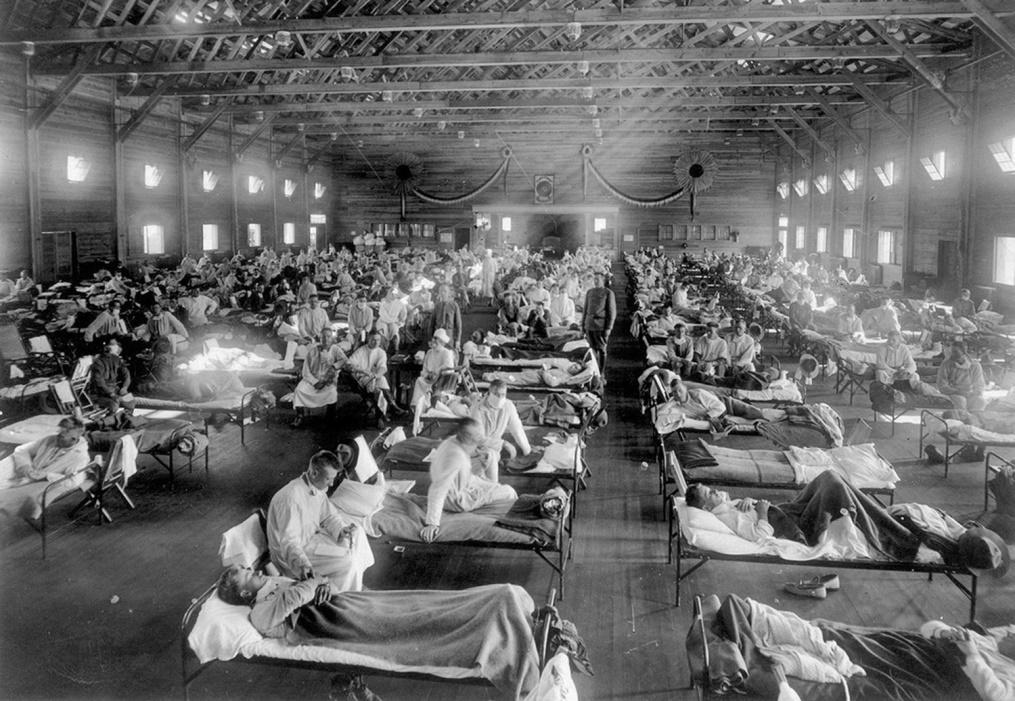
As the situation grew worse, governmental authorities were slow to react—that was a mistake. By late September 1918, the influenza virus had mutated into an extremely contagious and ruthless killer. This second strain swept rapidly across continents reaching not only densely populated cities and battle zones, but even the remotest regions of the earth, leaving more dead in its shadow than at times could be buried. As with all influenza, the virus attacked the victims’ respiratory systems. At first they coughed and wheezed. Before long, they gasped for air as the virus damaged and scarred their lungs, filling with fluid and blood that couldn’t be coughed up quickly enough. Many of the influenza victims died within days, some within hours. A person might appear perfectly normal that morning and be dead before nightfall. Crowds gathered at hospital doors begging admittance for them or their loved ones, merely to be turned away. Not only were all hospital beds taken, but cots with sick and dying stretched down hospitals’ hallways and into basements. As soon as victims succumbed to the disease, others took their beds, still warm and contaminated. Communities pitched army tents on the outskirts of town to act as temporary hospitals, but even that wasn’t enough.
In October at the influenza’s infectious zenith, the Surgeon General of the U.S. Army observed that the disease was killing not only the elderly and infirm, but the young and healthy. He alarmingly reported: “If the epidemic continues its mathematical rate of acceleration, civilization could easily disappear from the face of the earth within a few weeks.” Some in the United States couldn’t accept the pandemic as godsent and instead blamed their enemy Germany: “It is quite possible that the epidemic was started by Huns sent . . . to turn loose Spanish influenza germs,” reported the Chicago Tribune.
As if things weren’t sufficiently grave, profiteers, hoarders, and snake oil salesmen swooped in to exploit people’s fear and hopelessness. Newspaper advertisements, sometimes cast as news reports, promoted tonics “to prevent Spanish influenza” that act as “red blood builders” to “tone up and strengthen the organs of the body.” Others sold influenza masks and staples like sugar, flour, and grain at exorbitant prices while others hoarded more than they could use to the detriment of those who desperately needed them. The U.S. Food Administration tried to shame the profiteers and hoarders by describing them as “selfish, cowardly, unpatriotic” who were “taking unto one’s self special privileges at a time when all Americans should be on the same footing, share and share alike.” It did little. Fortunately, war-time laws already in place helped to curb many abuses. Through the worst of the outbreak, however, the U.S. economy and stock market remained relatively stable. The war had already severely affected supply and demand, distribution, and employment so there was little more damage to be done.
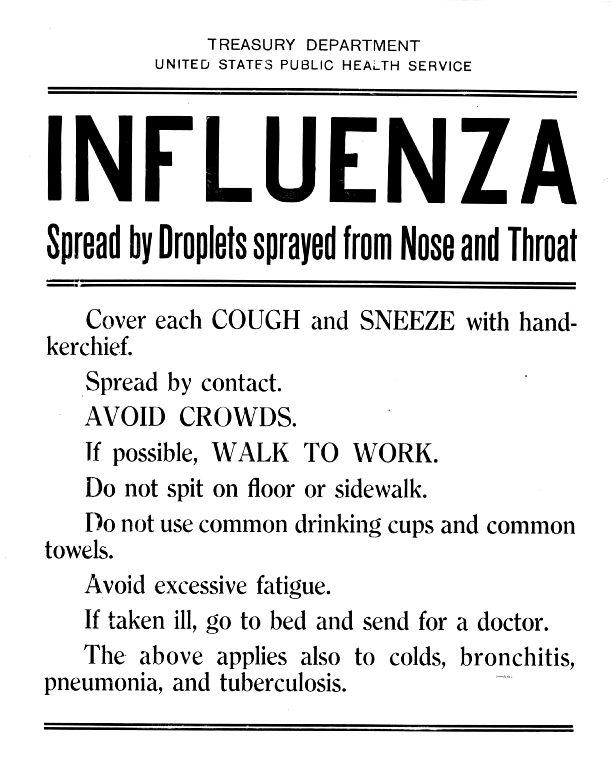
As the death toll mounted, newspaper headlines and articles captured the civic response that had taken hold at last: “Influenza Cancels Entertainment Plans;” “Influenza Puts Stop to Sports;” “Influenza Causes Churchless Sunday;” “[A]ll theatres, moving picture shows, dance halls, and all other unnecessary places of public assembly are closed.” Cities posted strict quarantines that “close[d] all stores except food and drug stores . . . office buildings also are affected.” Boards of Health distributed bulletins advising people to wear masks, stay at home unless absolutely necessary, and wash their hands. Some health bulletins even recommended that people “avoid talking about it” and to “keep an optimistic air about yourself.” Anti-spit ordinances were strictly enforced. In some cities, citizens caught not wearing masks in public were fined.
Even U.S. President Woodrow Wilson had fallen ill and delirious while at the Paris Peace Conference, though the public wasn’t told. His personal physician wrote from Paris that: “The President was suddenly taken violently sick with the influenza at a time when the whole of civilization seemed to be in the balance.” President Wilson recovered in time to help negotiate and sign the Treaty of Versailles that finally ended the most deadly war in history up to that time. Countries around the world celebrated with parades and parties in the streets, notwithstanding that influenza was still claiming lives. By early 1920, however, the pandemic had mercifully ended, too.
Many scientists and historians believe that 500 million people or close to one-third of the world’s roughly 1.8 billion inhabitants had been infected. Of those, an estimated 50 million people died from the virus and its secondary bacterial infections like pneumonia and staph. Antibiotics had yet to be discovered. The application of simple math produces a fatality rate of 10 percent of those infected or roughly 2.8 percent of the world’s population. Others put the statistics at twice those amounts. However you figure it, the Spanish influenza was the most deadly pandemic since the Black Death (bubonic plaque) of the 14th century. In the United States alone, an estimated 675,000 of the 103-million populace died. Not only does that exceed the number of American soldiers killed in World War I, but also the total number of Americans killed in all U.S. military engagements during the 20th century (e.g., WWI, WWII, Korea, Vietnam, Iraq, and Afghanistan).

Though seasonal influenza was common at the time, the Spanish flu was a novel H1N1 strain of influenza A not recognized by the human body. It was of avian origin caused by a virus jumping from a bird to a human, a rare occurrence called an antigenic shift or spillover event. Most pandemics are caused by antigenic shifts of influenza virus that become highly contagious. Influenza pandemics have occurred only four times in the last 100 years—the 1918 Spanish flu (H1N1), 1957 Asian flu (H2N2), 1968 Hong Kong flu (H3N2), and 2009 swine flu (H1N1). Today, a new pandemic is sweeping the world, originating not from an influenza virus, but from the coronavirus.
In December 2019, reports crept into the international news of an outbreak of flu-like symptoms and pneumonia emerging from China’s seventh largest city, Wuhan, in the Hubei province. Chinese authorities isolated the cause to a new coronavirus that jumped from an animal to a human perhaps at a large seafood or wild animal market. The mutated virus then began its rapid transmission between humans. The highly contagious virus has been named “severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2) and the resultant disease is called “coronavirus disease 2019” (COVID-19). The coronavirus is a family of hundreds of viruses that cause many respiratory illnesses ranging from the common cold to SARS. Because the strain of coronavirus that emerged from Wuhan is new and because all known influenza viruses are distinct from the coronavirus, no vaccine currently exists to prevent COVID-19.
As the health and economic impacts of COVID-19 continue unfolding, the pandemic is uncannily evocative of the Spanish influenza of 1918. Though the terminology has changed (social distancing, self-quarantine, flattening the curve), the nonpharmaceutical practices are much the same. Newspaper articles from 1918 advised the populace to engage in good daily health practices just as the Center for Disease Control (CDC) advises today: “everyone clean your hands often, avoid close contact, stay at home if you’re sick, cover coughs and sneezes, wear a facemask if you are sick, and clean and disinfect.” This is especially important since a recent joint study by the National Institutes of Health, CDC, and others found that the virus responsible for COVID-19 was detectable in aerosols for up to 3 hours, up to 4 hours on copper, up to 24 hours on cardboard, and up to 2 to 3 days on plastic and stainless steel.
Also painfully familiar when looking back to 1918 are the greed and selfishness of price gougers and hoarders whose target today is not sugar and flour as during the Spanish influenza, but hand sanitizer and toilet paper. Then there are those who make ridiculous and unproductive accusations, not against Germany as in 1918, but against China, North Korea, or the U.S. for causing today’s pandemic.
Yet, there are many circumstances in the United States today that are much more favorable than in 1918. We are not in the midst of a world war with scarce resources as were those suffering from the Spanish influenza. Moreover, our medical technology, healthcare infrastructure, and knowledge of how viruses develop and mutate are much more advanced than in 1918. Though there is no vaccine for COVID-19 so far, scientists around the world are working to develop one as quickly as possible. They also are testing an array of existing medications “off label” to treat COVID-19. Under the Defense Production Act of 1950 that can be invoked, private companies can expand and accelerate the production of indispensable medical supplies and equipment. Perhaps most importantly, we have antibiotics not in existence in 1918 to fight the bacterial complications that can often be deadlier than the virus.
So, here we are in the United States, a century after the Spanish influenza pandemic not knowing what to expect from this strain of coronavirus that has descended upon us. Will it burn out soon or will it mutate into something even more dangerous? What we do know is that many are being infected every day and thousands are dying, particularly those who are at high risk. Countless have been hurt financially from the plummeting stock market, from reduced or terminated wages and revenue, from price gougers and hoarders, and from the lack of freedom of movement. The news changes daily. Still, all is not bad news. Though Italy is facing its worst crisis since the end of World War II, China recently announced that no new cases are coming out of the Hubei province where the outbreak began. Hopefully, with the prevention and treatment techniques we’re currently implementing to moderate the spread of COVID-19, the curve will not only flatten like in China, but descend. No doubt there will be tough days ahead, but the news will eventually get better. To quote a cliché that is often overused during bad times, but is nonetheless applicable: This too shall pass.
PHILIP JETT is a former corporate attorney who has represented multinational corporations, CEOs, and celebrities from the music, television, and sports industries. He is the author of The Death of an Heir: Adolph Coors III and the Murder That Rocked an American Brewing Dynasty.